|
|
|
|
Advanced
Perfusion Settings (Advanced Options)
The Analysis Tab
Raw
dynamic curve analysis:
Note
that, in the absence of AIF deconvolution, the resulting ‘blood flow’ map is
only a very crude approximation, since the dispersion of the tissue response
due to a finite duration of the AIF is not accounted for. The Segmentation
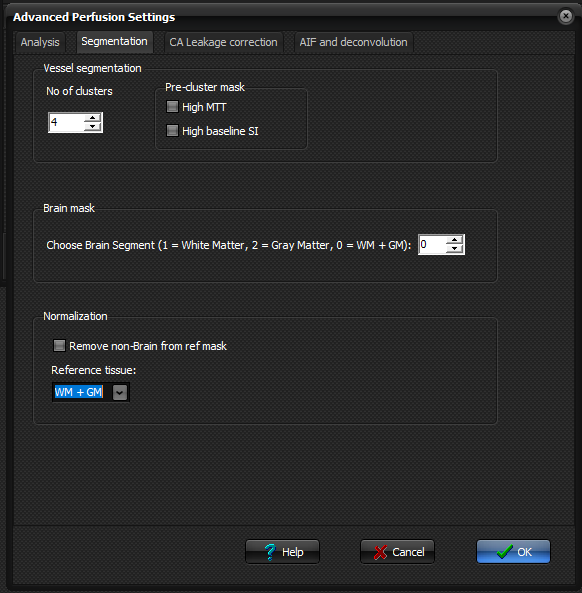
Tab
Tissue
segmentation is used for various purposes as part of advanced perfusion
analysis. All segmentation described here are based on segmentation of the
raw perfusion data using different properties of the dynamic signal response
or baseline signal intensity to group tissues into different clusters based
on predefined properties.
Vessel segmentation Number
of clusters used for the analysis can be specified. You can also choose to
remove areas with high MTT values and/or high baseline signal before the
clustering analysis is done.
Brain mask Select
which area you would like to use as the brain mask; white matter, grey matter
or both. This choice will be reflected in the Brain Mask output map selected
in Perfusion Settings. Normalization Choose
reference tissue, either white matter, grey matter or both. The resulting
mask is used as normal tissue for the normalization of CBV and CBF values to
normal tissue. If ‘remove non-brain from ref mask’ is checked, then bright
regions (assumed to represent pathology) in the raw baseline data (before
contrast agent arrival) is assumed to represent pathology and will be
clustered out. Note that this option is only applied to T2/T2*-weighted DSC
sequences, which are assumed to be sufficiently T2-weighted to render
pathology hyperintense relative to normal tissue. If no pathology is present,
then this option may result in undesirable effects by removing bright regions
of normal brain tissue, and the option should therefore be used with caution.
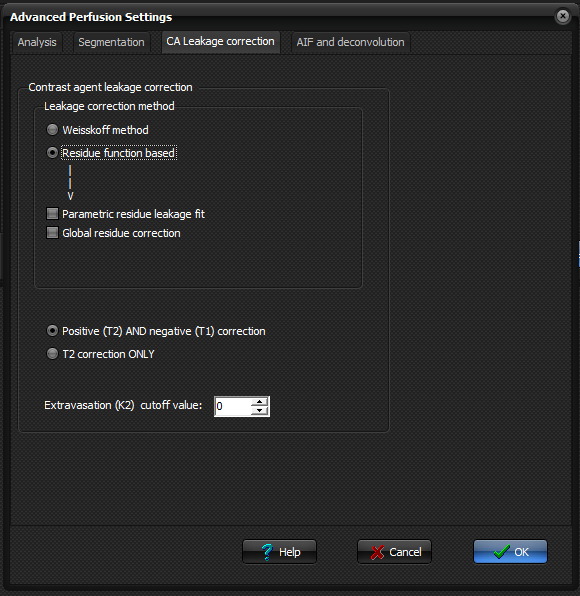
The CA Leakage Correction Tab
The
underlying kinetic model used in the perfusion module assumes that the
contrast agent is contained in the intravascular space for the duration of
the dynamic acquisition. If the blood brain barrier is severely compromised
due to pathology this assumption may no longer be valid. When <Apply
apply contrast agent leakage correction> is checked in the main menu, contrast
agent leakage from the intravascular to extracellular space is corrected for
using one of the two methods available in the Advanced Perfusion Settings
menu. Note that the leakage correction algorithms uses both WM and GM as
reference mask, regardless of the brain mask / normalization settings.
Two
methods for leakage correction exist:
When
leakage correction is enabled an additional output image can be generated
('Leakage map' or K2-map). This is a 'pseudo Ktrans' where the pixel
intensity is proportional to the rate of contrast leakage from the intra- to
the extravascular space. Detect both positive (T2) and negative (T1) K2 values: When
set, the leakage correction includes leakage causing both T1 and T2 effects
and hence does not depend on the 'tail' of the dynamic curve being negative
in leaky pixels. K2 cutoff: Leakage values (in terms of the
leakage constant K2) with an absolute value below the specified limit will be
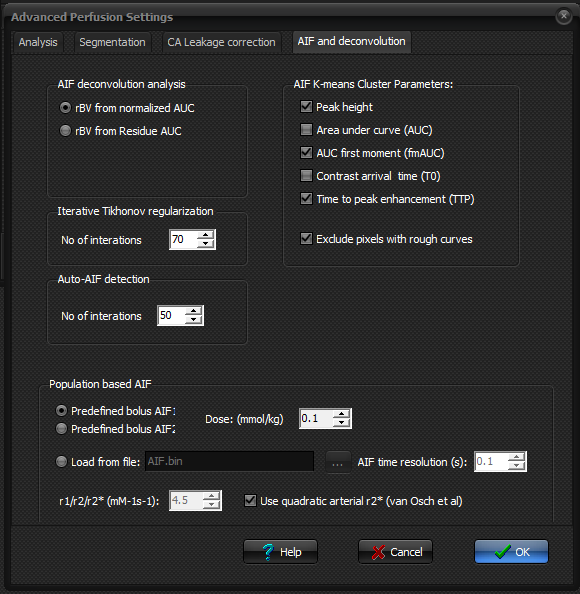
set to zero. The AIF and
deconvolution Tab
AIF deconvolution analysis When
AIF (arterial input function) deconvolution is applied the cerebral blood
volume can be estimated in two different ways as specified below: · rBV
from normalized AUC: The blood volume is estimated
by the normalized area under the dynamic curve; that is the area under the
tissue response curve divided by the area under the AIF. This is the most
common method for estimating the BV when the AIF is known. · rBV
from Residue AUC: Selecting this method, the BV
is estimated from the area under the residue function curve where the residue
function is estimated by AIF deconvolution. This method of determining BV may
be theoretically more correct but is also more sensitive to noise and to the
choice of deconvolution method. · Iterative
Tikhonov regularization o Here you specify the number of iterations to
run when the optimal singular value filter factor is determined iteratively
for Tikhonov regularization. The iterative procedure searches for the
'optimal' trade-off between a 'correct' solution and an oscillating solution.
For details of the method, see Hansen HC (SIAM Journal on Scientific
Computing 1993;14(6): 1487 – 1503). · No. of
iterations: This is the total number of iterations used to determine
the optimal regularization value. Note that if a large number of iterations
are used, the deconvolution analysis is significantly slower than when a
fixed threshold in used. Auto-AIF detection Specify
the number of iterations when the AIF is found automatically. AIF K-means Cluster Parameters Here,
you can specify the criteria to be used when performing an automatic search for
AIF. Changes to these settings should be done with caution, but some
optimization may be required for cases where default settings fail to provide
good estimation. Population based AIF Two
different shaped population-based AIFs are included. When 'Population based
AIF' is selected in the main menu of the perfusion module, the application
will use the AIF specified here. A ‘population based AIF’ as used here is a
standard AIF derived from a multi-compartment kinetic model of the expected
shape of a contrast bolus in the brain following a rapid injection in a
‘standard’ person. The kinetic model used to obtain the standard AIF is
described in van Osch MJ et al. Magn Reson Med. 2003 Sep; 50(3): 614-22. The
two different pre-defined AIFs differ in sharpness and maximum amplitude.
|
|
||
|
|
|
|